Sudden cardiac arrest in athletes: What we know or don’t know

On 2 Jan 2023 during a televised National Football League (NFL) game, 24 years old professional American Football player Damar Hamlin collapsed on the field due to a sudden cardiac arrest (SCA). He was attended to within seconds and cardiopulmonary resuscitation (CPR) and automated external defibrillation (AED) were both administered on field. After 9 days in hospital, Mr Hamlin was discharged, and less than 2 weeks later on 23 Jan 2023, made his first public appearance since his collapse as a spectator.
Another instance of sudden cardiac arrest during a televised sport was that of Danish footballer Christian Eriksen during the UEFA Euro 2020 tournament on 12 Jun 2021. Mr Eriksen suffered a cardiac arrest during a live match and required prompt CPR and AED administration. Aged 28 years old at the time of collapse, Mr Eriksen made a full recovery and was subsequently fitted with an implantable cardioverter-defibrillator (ICD). He is currently still playing competitive football in the English Premier League.
What is sudden cardiac arrest?
SCA is an electrical malfunction whereby the heart rhythm becomes extremely abnormal unexpectedly such that the heart stops pumping. This causes the blood supply to vital organs such as the brain and lungs to be cut off, leading to sudden collapse. If not treated within seconds, death may occur.
How common is sudden cardiac arrest in athletes?
SCA is rare in athletes. Depending on country and level of sport, one in 50,000 to one in 15,000 athletes may be affected. In athletic individuals, the frequent and constant training to physical limits as well as training environment may interact with pre-existing heart conditions or give rise to new life-threatening situations that may eventually lead to SCA.
What are the conditions that lead to sudden cardiac arrest?
These can be divided into 2 large groups based on age.
For young athletes aged 35 years and below, there are 3 main categories of heart conditions that predispose to SCA. These are:
- Structural heart conditions such as
- Hypertrophic cardiomyopathy, a condition where the muscle fibres of the heart grow and multiply in an abnormal fashion
- Arrhythmogenic cardiomyopathy, a condition where the muscular portion of the heart is replaced by abnormal tissue, affecting the heart rhythm and function
- Anomalous coronary artery, a condition where the blood vessels that supply the heart muscle originate from abnormal locations
- Electrical abnormalities such as long QT syndrome and Brugada syndrome
- Acquired conditions such as myocarditis (infection of the heart muscle) and commotio cordis
For master athletes aged above 35 years, the most common cause of SCA is atherosclerotic coronary artery disease.
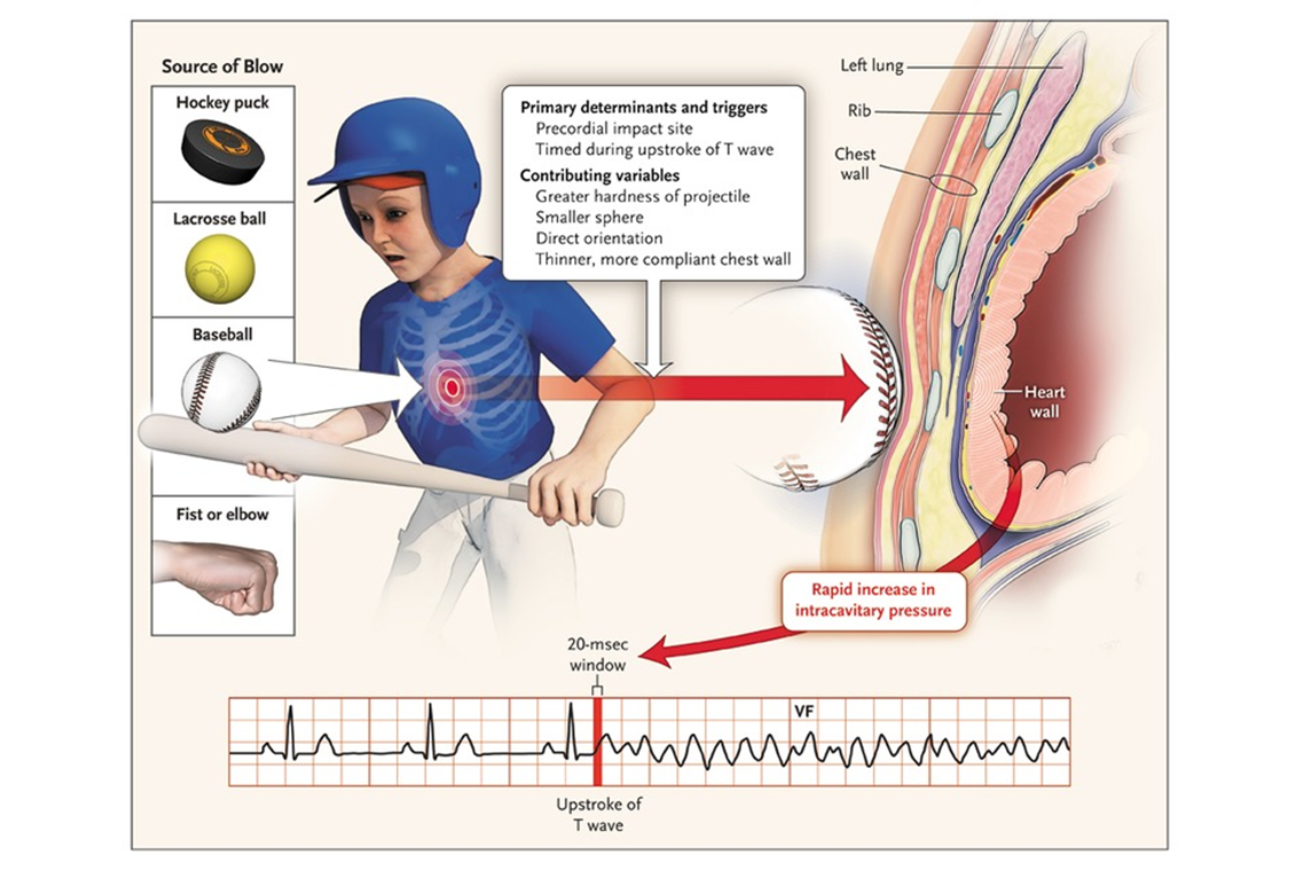
What is commotio cordis?
While the exact cause of collapse for Damar Hamlin has not been revealed, a lot of speculation has centred around commotio cordis (“agitation of the heart” in Latin) as a likely culprit. This condition tends to occur in much younger athletes, as more than 90% of documented cases were aged below 25 years.
A typical scenario in commotio cordis involves a small projectile (commonly a baseball or hockey puck) striking the heart at a very precise timing within the electrical cycle. This disrupts the electrical stability of the heart and triggers a life-threatening abnormal heart rhythm called ventricular fibrillation, leading to SCA.
 1
1
Is there a role for screening?
Yes. Pre-participation screening involves answering a detailed questionnaire to pick up potential warning signs for SCA, such as unexplained passing out, dizziness, chest pain and shortness of breath. It also includes determining if there is a family history of conditions that may increase the risk of SCA.
In selected situations, a resting electrocardiogram may be performed to screen for suspicious electrical signals. For those above 35 years old, it is also important to screen for typical cardiovascular risk factors such as high blood pressure, high blood cholesterol and diabetes, all of which may increase the risk of atherosclerotic coronary artery disease.
Depending on the results of the pre-participation screening, your cardiologist or sports physician may arrange for further tests as necessary before allowing you to participate in sports. However, screening is not foolproof and some conditions may not be detectable at the time of screening. Moreover, mass screening requires substantial resources and may not be feasible at all levels of sport.
What else can be done in such situations?
Early recognition, early CPR and early defibrillation are absolutely crucial for any instance of SCA. SCA has to be suspected in any case of sudden collapse or loss of consciousness, with immediate checking of pulse and initiation of CPR if the pulse is absent. In certain cases, the individual may appear to be gasping but this should not be mistaken for him or her being conscious. On the contrary, gasping is a form of involuntary response in someone with SCA. Prompt administration of an AED will allow life-threatening heart rhythms to be detected and treated with defibrillation.
Time is of the essence and every second counts in SCA. Early recognition and bystander CPR and AED substantially increases survival for those with SCA. On the contrary, delays will significantly increase the risk of brain damage and death.
Conclusion
Sudden cardiac arrest is a devastating event and can happen even in the fittest individuals. While it is a very rare occurrence, we can still do our part to minimise it. Appropriate pre-participation screening as well as CPR and AED training will help in detection of potential life-threatening conditions and prompt treatment in cases of collapse respectively.
Be trained in CPR+AED now by signing up for one of our lifesaving courses here.
Article is contributed by Asst Prof Yeo Tee Joo, Board Member of the Singapore Heart Foundation and Senior Consultant, Department of Cardiology at the National University Heart Centre, Singapore.
References:
- Maron, B. J., & Estes, III, N. M. (2010). Commotio Cordis. The New England Journal of Medicine. https://www.nejm.org/doi/full/10.1056/NEJMra0910111


")

