What is Aortic Valve and Aortic Stenosis?

The aortic valve functions like a “one-way door”, allowing the heart to supply essential oxygenated blood to the body’s tissues and vital organs. However, as we age, the aortic valve could undergo change, becoming hardened, thickened, and narrowed – a condition known as aortic stenosis (AS). The constriction impedes the efficient flow of blood from the heart to the vital organs, and is a serious medical condition which must not be overlooked.

Figure 1: The pathway of blood flow through the heart
Unlike the mitral valve, which serves as the heart’s entry point (as illustrated in Figure 1), the aortic valve serves as the exit, regulating blood flow from the main heart pumping chamber, the left ventricle. A comprehensive assessment, including a physical examination by a doctor, and advanced diagnostic investigation, such as the use of ultrasound evaluation by echocardiogram (as shown in Figure 2), is crucial for determining if the afflicted valve is diseased, and for gauging the extent and severity of the valve dysfunction.
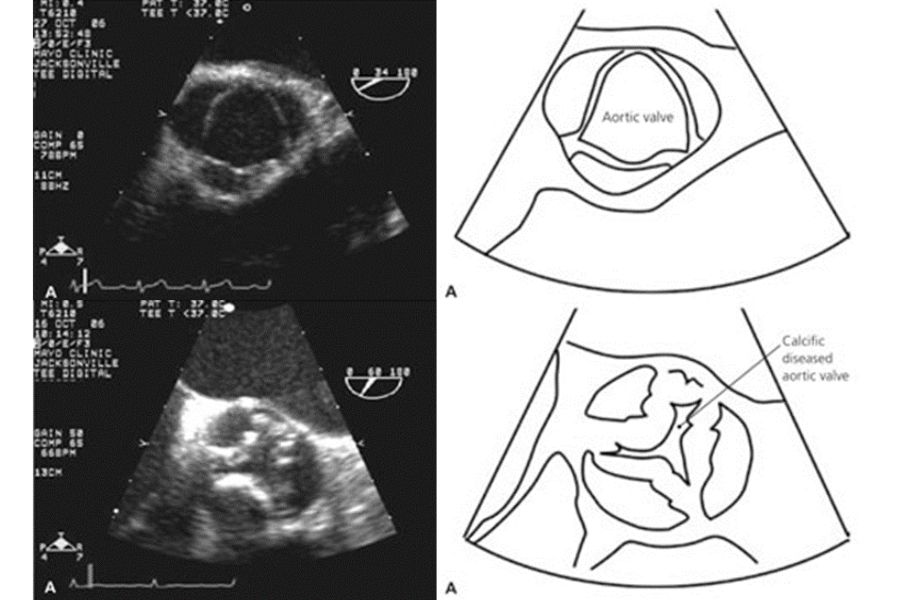
Figure 2
The most common cause of AS stems from the natural wear and tear of the aortic valve, particularly in the elderly (as illustrated in Figure 3c). In less frequent instances, AS may result from previous infections affecting the aortic valve, such as in rheumatic heart disease (Figure 3d), or from congenital abnormalities where individuals are born with deformed aortic valves, known as bicuspid aortic valves (Figure 3b). Unfortunately, there is currently no proven treatment which prevents or delays the progression of AS.
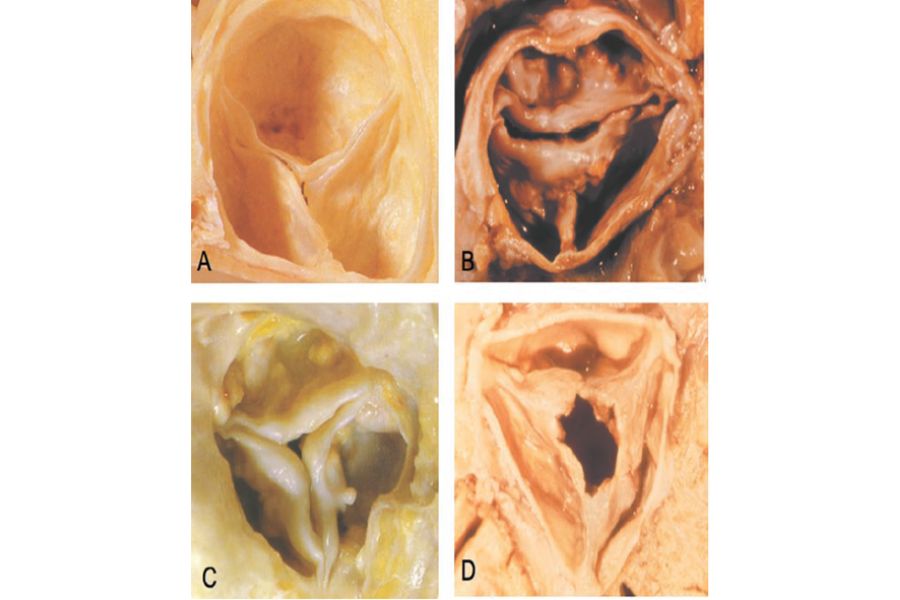
Figure 3: Aortic Stenosis Causes
When the aortic valve narrows significantly, vital organs may receive insufficient blood supply, especially during physical exertion such as exercise. This could manifest in symptoms commonly associated with severe AS, including chest pain, fainting, or breathlessness.
The prevalence of AS is on the rise among Singapore’s ageing population. It is estimated that moderate or severe AS exists in 3% of individuals who are over 75 years old, and 8% in those over 85 years old.
Treatment Options for Aortic Stenosis
The treatment options for AS range from medication to alleviate symptoms, to surgical procedures to repair or replace the damaged valve. Once a patient has advanced to severe AS, medical treatment alone is usually insufficient, and the patient faces a high risk of mortality; approximately half of these patients pass on within one to two years, if they are left untreated.
Surgical interventions come in the form of conventional open-heart surgery, and less invasive methods. An open-heart surgery is a well-established response to replace the damaged aortic valve with an artificial aortic valve (as depicted in Figure 4). However, it is important to note that not all patients are fit for this surgical option; the most vulnerable are the elderly and those with multiple health conditions.
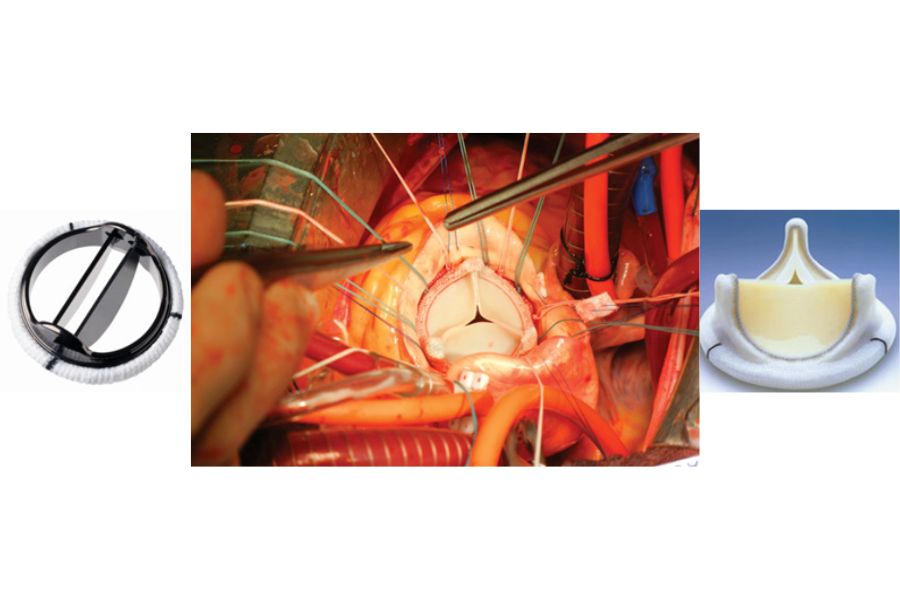
Figure 4: Surgical Aortic Valve Replacement
With the advancement of valve therapies, less invasive treatment such as Transcatheter Aortic Valve Implantation, has emerged as a viable alternative for patients with severe AS, and are unsuitable for conventional surgery. The Transcatheter Aortic Valve Implantation (TAVI) is a lifesaving solution.
Transcatheter Aortic Valve Implantation and Post-Procedural Care
Transcatheter Aortic Valve Implantation
TAVI is a minimally invasive procedure, performed by inserting a catheter with a tissue stent valve, into the major artery of the thigh. This procedure is typically carried out under local anaesthesia and sedation.
Before the procedure, the patient is required to undergo a computed tomography (CT) scan. This imaging study allows the surgical team to plan and determine the optimal route for the stent valve to reach the heart.
During the procedure, the stent valve is positioned across the narrowed aortic valve to displace the damaged valve, thereby enhancing the flow of blood from the heart to vital organs. Within the stent are biological valve leaflets which take over the crucial role of the original aortic valve (as illustrated in Figure 5 and 6). The procedure usually takes less than an hour, after which the patient is moved to the intermediate care area for an overnight monitoring. The following day, the patient is transferred to a general ward and is expected to be able to return home within one to two days.

Figure 5: TAVI Valve
![]()
Figure 6: Transcatheter Aortic Valve Implantation
Post-procedural care
After the TAVI procedure, patients undergo continuous monitoring in the hospital to check for complications and to ensure that the new valve functions effectively. They also undergo rehabilitation to improve post-surgery mobility so as to enhance their recovery.
Patients are required to take blood-thinning medication such as aspirin. Generally, they could resume regular activities approximately one week after surgery. It is essential for post-TAVI patients to note that they require antibiotic prophylaxis for invasive dental treatment.
Faster and better recovery
The availability of advanced valve treatment therapies such as TAVI has offered a lifeline for patients with severe AS and are unable to undergo conventional open-heart surgery. The minimally invasive procedure not only enables patients to recover faster and in a shorter hospital stay, but also demonstrate that they are able to get back to their normal lives earlier.
| Heart Valve Disease Heart valve disease is a disorder of the heart valves, the tissue flaps that regulate the flow of blood in and out of the heart chambers. Patients with heart valve disease usually have one or more damaged heart valves. The most common heart valve diseases are AS and mitral valve regurgitation. In mitral valve regurgitation, the mitral valves which bring oxygenated blood from the lungs to the heart, are unable to close properly, causing blood to flow backwards. This causes insufficient blood to be pumped to the rest of the body, and as a result, the patient is fatigued and breathless. Find out more about mitral valve disease and its treatment here. In addition to the stipulated valve diseases, there are also lesser known but increasingly common valve ailments such as tricuspid valve regurgitation that could affect the major organs and result in poor quality of life. |
Article and images are contributed by Asst Prof Ho Kay Woon, Senior Consultant at the National Heart Centre Singapore.



