Diagnosis and Treatment

Non-invasive Tests
Blood Tests

Substances like creatinine kinase and troponin are released into the bloodstream when the heart is damaged during a heart attack. Blood tests to detect the presence of these substances are useful in helping doctors confirm a heart attack or estimate the time of an attack. They also help detect any injury in the heart muscle due to a heart attack.
Chest X-ray

An X-ray of the chest reveals basic information about the size and shape of the person’s heart, blood vessels, and lungs.
Electrocardiography / Electrocardiogram (ECG)

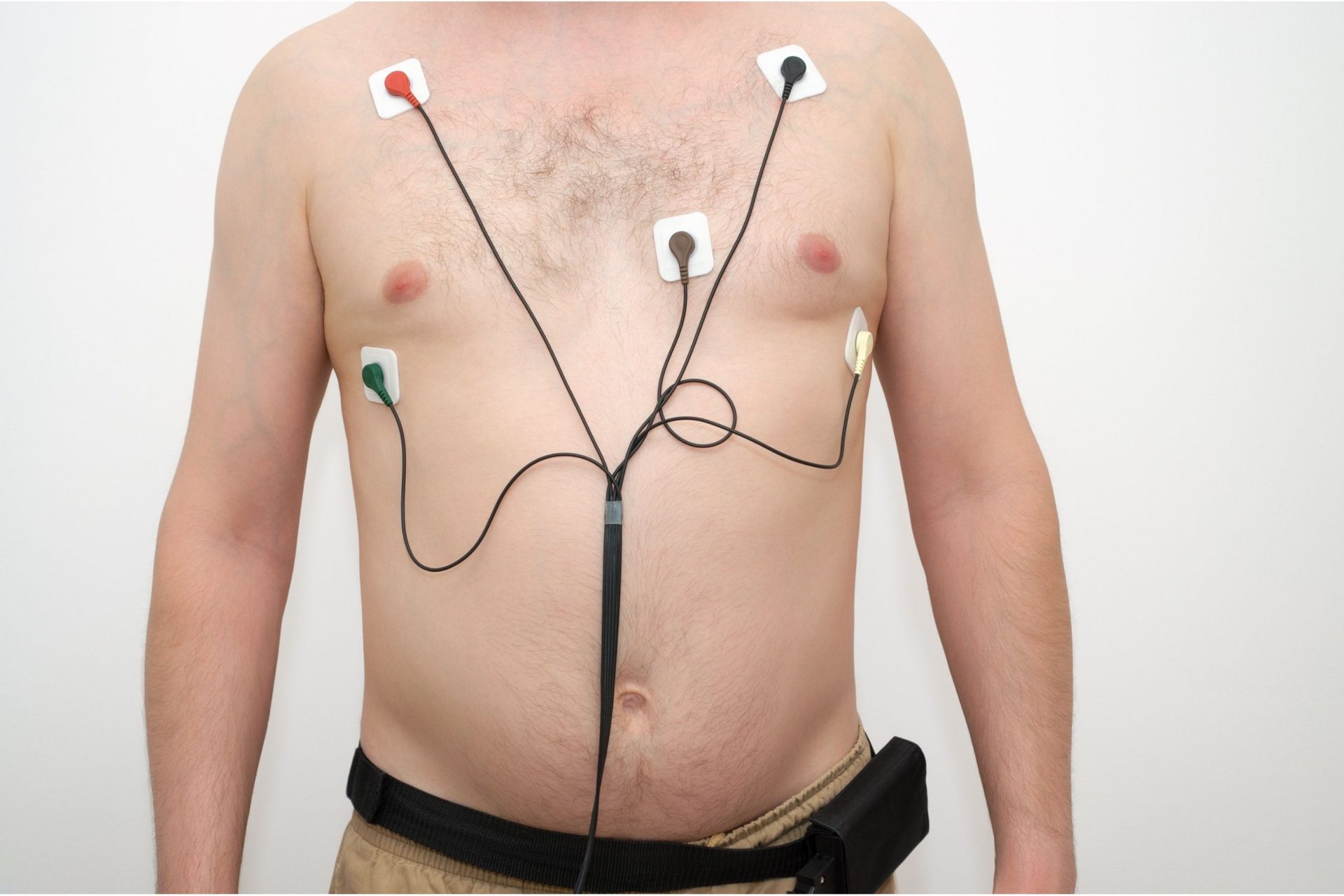
Electrocardiography (ECG) is a method of measuring the electrical activity in the heart. It is a diagnostic test where 12 electrodes (small patches) are attached to your arms, legs and chest, and connected to a machine to record the rhythm and electrical activity of the heart.
The test takes about 10 minutes to complete. The printed result – an electrocardiogram (ECG) – contains information about the patient’s heart rhythm, heart rate, electrical abnormalities, and thickening of the heart muscle. It can also show any previous or ongoing heart attack and if blood supply to the person’s heart is poor.
Together, these data provide clues to the likely reasons for the patient’s cardiac condition and the appropriate course of treatment.
Holter Monitoring
Holter monitoring is ECG monitoring done over 24 hours or longer, usually in the course of a normal day’s activities. The patient carries a small ECG monitor in a pouch worn on his/her body to take measurements at spontaneous periods of chest pains and/or irregular heart rhythms that he/she may experience during the test period.
Exercise Stress Test

Typically, the patient will run on a treadmill wearing the usual ECG electrodes. Recordings are taken simultaneously at 3-minute intervals, with the speed and elevation of the treadmill increasing gradually. This will continue until his/her target exercise heart rate is reached or the patient develops chest pains and is unable to continue with the test.
An exercise ECG is most helpful for a patient who experiences chest pains only upon physical exertion but otherwise has normal ECG results when at rest. It allows doctors to assess the amount of physical activity the patient can endure. It also sheds light on how well his heart responds to the stress arising naturally from exercise.
Echocardiography

This technique uses sound waves (ultrasound) to assess the internal structure, movement, chambers, and valves of the patient’s heart. Further techniques such as Doppler echocardiography may also help highlight any disorders of the heart valves, coronary muscles and coronary arteries.
Computed Tomography (CT) scan

A CT scan is an X-ray procedure that produces cross-sectional images of the patient’s chest, including his heart and the surrounding blood vessels. It is useful in diagnosing cardiac tumors, aortic disease, and pericardial disease (disease of the pericardium).
Computed Tomography (CT) Coronary Angiogram
Similar to CT scan, this non-invasive test scans the coronary arteries with the intravenous injection of a dye to diagnose the cause of chest pain or other symptoms due to coronary arteries disease.
Patients may develop an allergic reaction to the dye used in the procedure, but that is not common, and doctors will assess patients’ situations accordingly. There is also some exposure to radiation during the test.
This procedure does not require recovery time.
Computed Tomography Calcium Score
Associated with the CT coronary angiogram study, a calcium score is measured preceding the CT angiogram. As the cholesterol fatty plaques in the arteries have the property of absorbing calcium from the blood as a chemical reaction, the calcium score will reflect the amount of plaques in the arteries. A high score indicates significant atherosclerosis in the coronary arteries.
The calcium deposits in the arteries are not related to your diet or any supplements you may be taking.
Magnetic Resonance Imaging (MRI)
In MRI, powerful magnets are used to produce three-dimensional, high-resolution images of the patient’s internal organs using a magnetic field. Such images, which include detailed information about the heart muscle, are vital in detecting damage caused by a heart attack, disease of the coronary arteries, and other cardiovascular defects.
Cardiac Nuclear Imaging
![]()
This is a diagnostic procedure where a small amount of radioactive substances known as radionuclides (for instance, thallium or rubidium) is injected into the patient’s bloodstream to check the blood flow through your heart using a camera. As the radioactive substances flow through the patient’s cardiovascular system, images are taken to detect how well the heart’s chambers are working, the blood supply to the heart, and if a heart attack has damaged any heart muscle.
Invasive Tests
Cardiac Catheterisation / Coronary Angiography
Cardiac catheterisation is commonly performed before invasive procedures such as “balloon” angioplasty to determine the type and extent of surgery required.
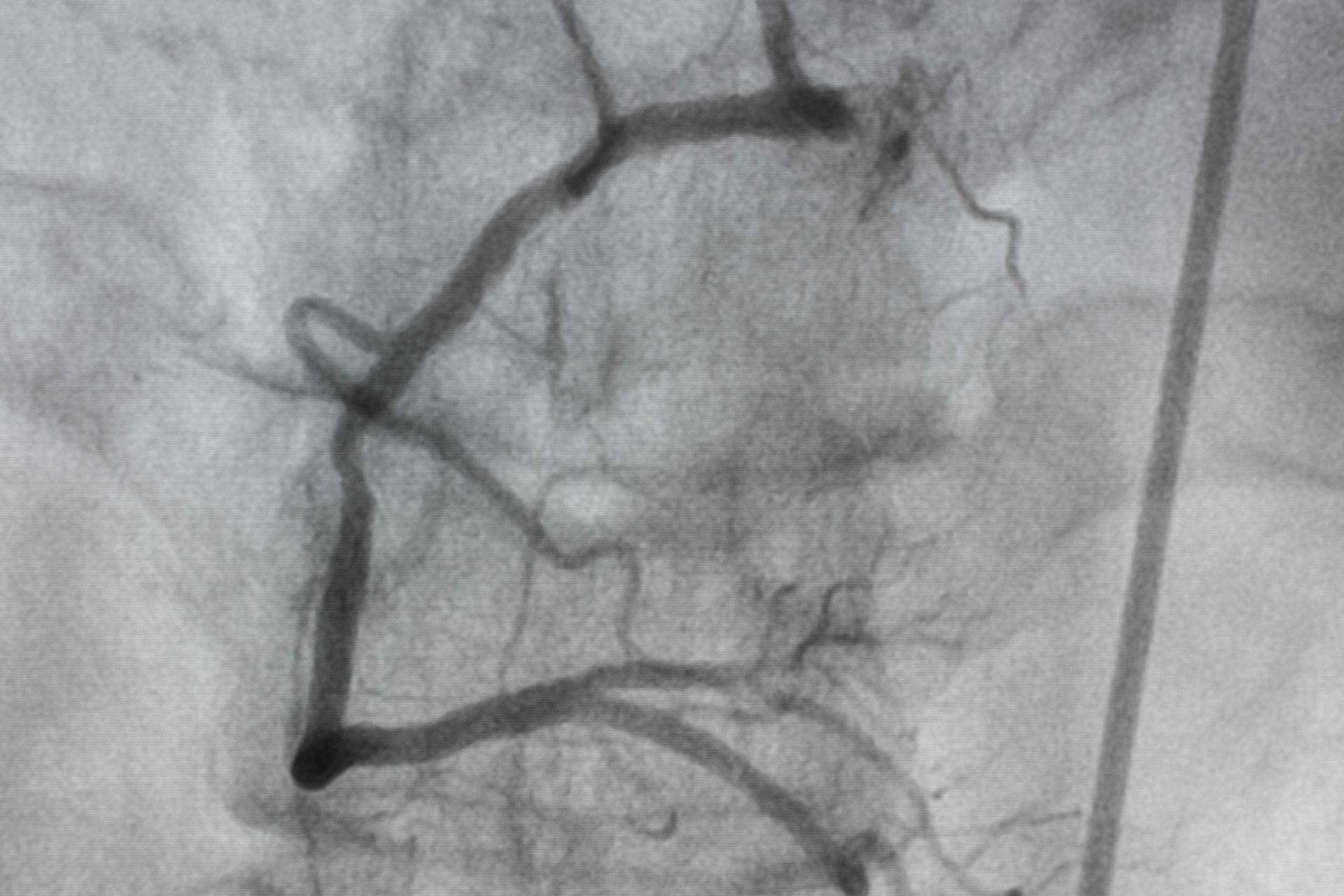
A dye is first introduced into the patient’s heart through a catheter inserted from the limb. X-rays are then taken as the dye moves through the heart to assess pressure and oxygen content in the cardiac chambers and the heart’s pumping ability.
The dye shows up as white lines on the X-rays, with disruption or narrowing of the lines indicating areas where the coronary arteries are obstructed.
Trans-Oesophageal Echocardiography
Trans-oesophageal echocardiography involves inserting an instrument into the patient’s throat and down the oesophagus (the tube connecting the mouth to the stomach). As part of the oesophagus lies close to the heart, the images captured by the ultrasound probe can give a very clear picture of the heart’s structure.
Electrophysiologic Study
Classification Of Heart Disease
Based on the results of the diagnostic tests, doctors usually classify a patient’s heart condition based on how severe his symptoms are. In this respect, the most used classification system is the New York Heart Association’s Functional Classification, which places patients into one of four categories depending on the extent to which their cardiac problems limit their capacity for physical activity.
| Class | Nature of Symptoms |
| I | No symptoms and no limitations on ordinary physical activities |
| II | Mild symptoms with slight limitations on ordinary activities. The patient is comfortable at rest. |
| III | Symptoms are sufficiently serious to place significant constraints on ordinary physical activities and less strenuous activities. The patient is comfortable only at rest. |
| IV | Symptoms impose severe limitations on the patient’s daily activities. The patient experiences symptoms even while at rest. |
Treatment
Depending on the symptoms and severity of the heart condition, various treatment options may be available. These range from non-invasive treatment such as medication if the patient’s symptoms are mild to invasive treatment if his condition is more serious.
Medication

Angiotensin-converting enzyme inhibitors – also known as ACE inhibitors – are commonly used to treat hypertension and congestive heart failure to reduce the narrowing effect on blood vessels.
Anti-anginal drugs – for instance, beta-blockers and calcium channel blockers (e.g. verapamil). These relax the muscles in the heart and blood vessels, thus alleviating the crushing chest pain of angina attacks.
Beta-blockers impede the action of hormones, such as adrenaline, which make the heart beat faster and more vigorously. Calcium channel blockers reduce the amount of calcium entering the muscle cells of coronary arteries, causing these vessels to relax and widen.
Anti-arrhythmic drugs – for example, amiodarone and flecainide. They are used to control disturbances in the heart rhythm.
Anti-coagulants – An agent that retards blood clotting but does not dissolve existing clots. It prevents new clots from forming and existing clots from becoming larger.
Blood clots consist of platelets (minute blood cells) and a protein called fibrin. Anticoagulants help to guard against blood clots by preventing fibrin from forming. They are often prescribed for patients with coronary heart disease who are especially vulnerable to thrombosis in their already-narrowed coronary arteries. Examples include heparin and warfarin.
Anti-platelet drugs – similar to anti-coagulants, they prevent blood clots. But unlike anti-coagulants, they do not target fibrin in the blood. Instead, they reduce the tendency of blood clotting by lowering the “stickiness” of the platelets in the blood.
Aspirin is the anti-platelet drug most prescribed. It is often recommended for patients with coronary heart disease or atherosclerosis and protects against ischaemic strokes.
Diuretics – used to treat patients suffering from congestive heart failure and have excessive amounts of water and salt in their bodies. Diuretics help to increase the output of water and salt in the urine.
The 3 main types of diuretics are Thiazide, loop diuretics and potassium sparing diuretics.
Invasive Treatment
Percutaneous Transluminal Coronary Angioplasty (PTCA)
Commonly known as “balloon” angioplasty, PTCA is a procedure to widen the coronary arteries that are blocked severely by an atherosclerotic plaque to restore blood supply to the heart muscle.
A catheter with a deflated balloon attached to its tip is inserted into an artery in the patient’s leg and then gradually manoeuvred to the blocked or narrowed section of the affected coronary artery. After the balloon is positioned across the most severe area of narrowing, it is inflated and deflated several times to squeeze the cholesterol deposits against the coronary artery wall. As a result, it widens the opening of the affected artery and improves blood supply to the heart.
In general, the procedure has a high success rate of approximately 90%, and the risk of major complications is low. However, the extent to which a blocked coronary artery is widened by angioplasty may vary significantly from individual to individual.
Stent placement often follows the balloon angioplasty to prevent re-narrowing of the artery.
Stent Implantation
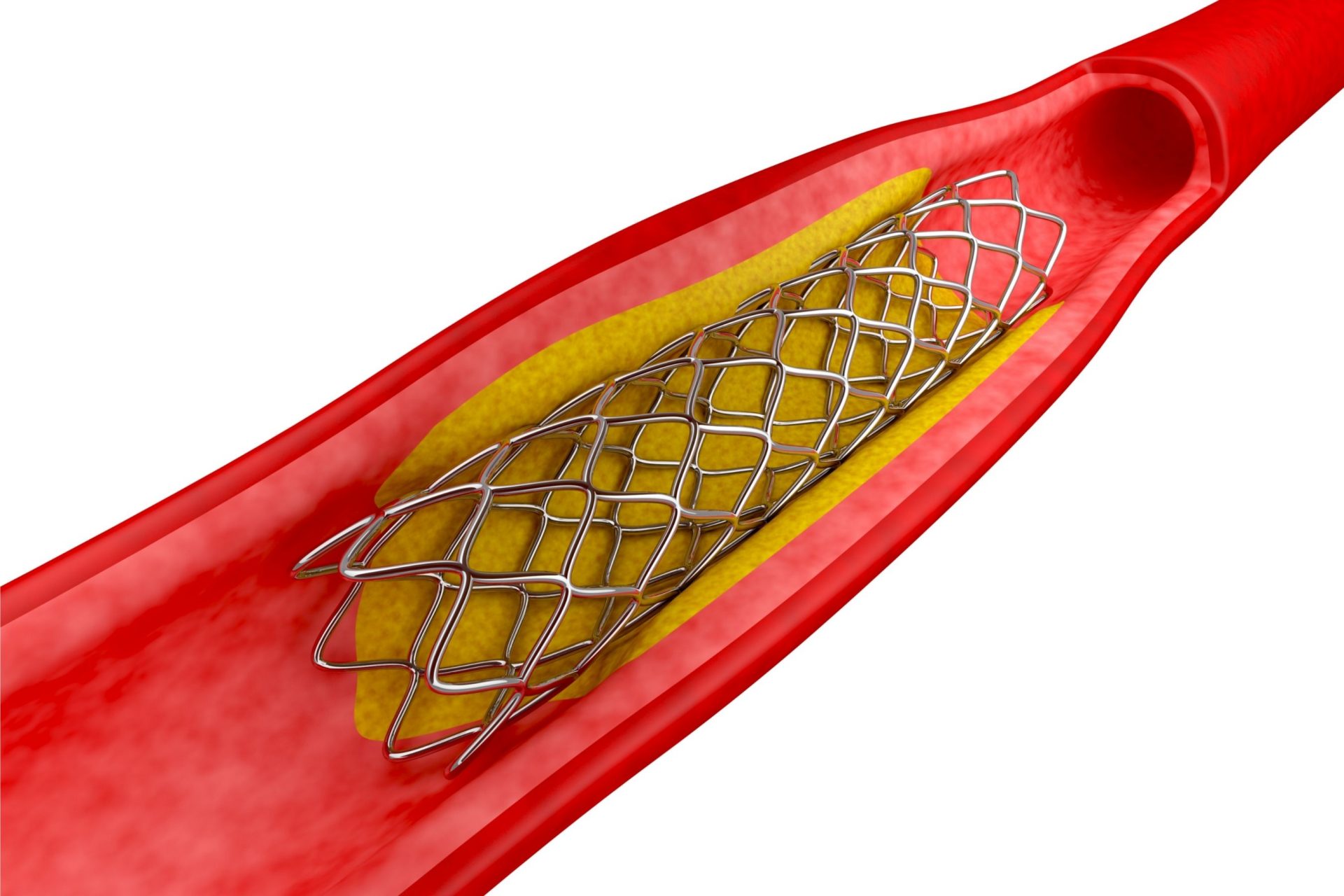
A stent, in the form of an expandable metal coil or mesh, is placed on an angioplasty balloon and guided to the blockage (similar to PTCA). The angioplasty balloon is then inflated to stretch open the stent and implant into the walls of the blocked artery.
Stent implantation also has a relatively high success rate of close to 90%. Patients who have undergone this procedure may subsequently have to take extensive blood thinners to prevent blood clots in their coronary arteries. The stent placement significantly reduces the chances of re-narrowing of the artery.
Percutaneous Coronary Intervention (PCI)
A non-surgical procedure used to treat the narrowing of coronary artery disease. The procedure involves combining coronary angioplasty and stenting.
Coronary Artery Bypass Grafting (CABG)
A patient with angina may not be a suitable candidate for angioplasty or stent implantation if he has atherosclerosis at several sites in his coronary arteries. In this case, CABG may be recommended.
This procedure involves creating a new route for blood to flow around the blocked part of each affected coronary artery. This is typically done by taking a section of a healthy blood vessel from another part of the body (for instance, the saphenous veins in the leg or the internal mammary arteries inside the chest) and using them as grafts to bypass the obstructed portions of the coronary arteries. The blood vessels chosen as grafts are usually extra vessels not affecting blood flow.
One end of the graft is attached to the aorta, and the other end to that part of the affected coronary artery, which lies downstream of the blockage. This way, oxygenated blood can flow through the coronary artery via an alternative route.
If more than one blockage is present in the patient’s coronary arteries, more than one graft will be needed. On average, a patient will require three to four bypass grafts. After the operation and upon recovery, the patient can expect a dramatic improvement in his cardiac condition.
More on coronary artery bypass surgery here.
Heart Valve Surgery
If a person has a damaged valve, the heart pumps blood around the body less efficiently. It is important to have these valves repaired or replaced in some cases so that the heart does not have to overwork.
A valve can be repaired by cutting, stretching, or sewing. If the valve cannot be repaired, it can be replaced with an artificial valve that can either be tissue or mechanical.
Transcatheter Aortic Valve Implantation (TAVI)
![]()
A TAVI procedure repairs the heart valve without removing the old and damaged valve. It may be done on patients who need an aortic valve replacement but are not well enough to undergo a heart valve surgery.
Somewhat similar to stent implantation, the TAVI approach delivers a replacement valve to the valve site through a catheter that passes through the heart from the thigh.
Once the new valve is expanded, it pushes the old valve leaflets out of the way, and the tissue in the replacement valve takes over the job of regulating blood flow.
Implantation of Electrical Devices
- A pacemaker is an electrical device inserted just beneath the skin to regulate the heartbeat in people with severe arrhythmia. It consists of a lead in a plastic tube, together with a metal core and a tip. The lead is inserted into the patient’s heart through a vein and then attached to a box with electrical circuits. Whenever the heart skips a beat, the pacemaker will emit a tiny electrical pulse to stimulate the heart and cause it to beat. A pacemaker can be either programmed externally or fitted with built-in sensors.
- A defibrillator is an electrical device used to restore normal heart contraction rhythms by delivering a carefully regulated electrical current to the heart when it suddenly stops beating effectively. Although defibrillators are usually used as external devices, they may sometimes be implanted within the patient’s body.
Heart Transplantation
![]()
Heart transplantation is an end-stage procedure carried out as a last resort only if the patient’s heart condition continues to deteriorate despite other forms of treatment to such an extent that his chances of survival drop to less than 50%.
This procedure involves replacing the patient’s diseased heart with a healthy heart from a donor, typically a person who has been medically certified to be brain-dead. The donor’s heart is completely removed and transported to the patient, who in turn has his diseased heart removed, leaving only the back walls of his upper chambers (the left and right atria).
The back part of the donor’s heart atria is opened up, and that heart is sewn into place by suturing its upper chambers to the recipient’s atria. Next, the blood vessels are connected, and blood flow through the heart and lungs resumes. As the patient’s new transplanted heart warms up, it begins beating. The patient is kept alive throughout the operation with a heart-lung machine that pumps blood to the rest of his body.
Not every cardiac patient suffering from end-stage heart disease is a suitable candidate for a transplant. In general, the patient must
- Have exhausted all other alternative forms of treatment
- Be likely to die if he does not have a heart transplant
- Be in good health generally apart from his cardiac condition; and
- Be able to tolerate the many lifestyle changes (for instance, following a regime of complex medications and frequent medical examinations) required after a transplant.
Patients who do not meet these criteria – in particular, patients with other existing medical problems such as insulin-dependent diabetes or impaired kidney function – are not good candidates for a heart transplant.
Heart donors are those whom doctors have declared to be brain-dead, meaning individuals whose brains show no signs of activity even though they are being kept physically alive by a ventilator. Donors tend to be people who have died from a traffic accident, severe head injury, or stroke. The ideal donor is one who
- Is under the age of 45
- Does not suffer from any significant heart disease
- Does not have risk factors for cardiovascular disease, cancer, or other acute or chronic illnesses
The blood group and weight of the donor must also match those of the intended recipient.
In the immediate aftermath of a heart transplant, the patient is closely monitored in an intensive care unit and remains on a ventilator for several hours until his condition stabilises. After that, the patient will generally be up and about within a few days. In the ensuing weeks, the risk of rejection of the newly-transplanted heart is high as the patient’s body will treat that heart as a foreign object. To tide the patient over this period, he will be prescribed immunosuppressants even though they will reduce his body’s natural defences against infections. Organ rejection and infection are most likely during the critical 1-month period following a heart transplant. After that, if the patient’s condition is relatively stable, he may be discharged from the hospital. Most patients will be discharged within 2 weeks.
In general, a successful heart transplant will dramatically improve the patient’s quality of life. The patient will be able to lead a more active life, including returning to work. He is, however, likely to have to take immunosuppressants for the rest of his life to prevent his body from rejecting the transplanted heart.




