Wearable Technology Enhances Atrial Fibrillation Detection and Monitoring

Atrial fibrillation (AF) is the most common rapid arrhythmia. It is estimated to occur in 1-2% of the Asian population, and increases to more than 10% in those who are older than 80 years old. It has also been estimated that at age 40, the lifetime risk of AF is 26% for men and 23% for women.
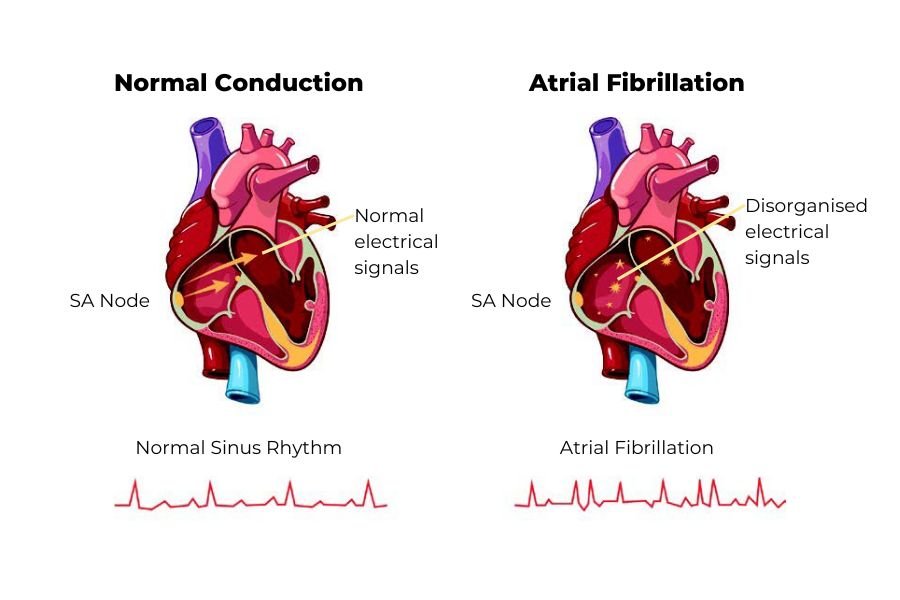
In normal circumstances, depicted on the left, the sinus node (SA node) passes signals to the ventricle to make it eject blood at regular intervals. In AF, depicted on the right, disorganised electrical impulses reach the ventricles, causing irregular heartbeats.
Complications of AF
AF leads to a very chaotic activation of the atrium, resulting in stasis of blood and hence clot formation. In the predisposed individual, this can cause thromboembolism (formation of a clot (thrombus) in the blood vessel that breaks loose and is carried by the blood stream to plug another vessel), and stroke.
In a Framingham study, approximately 20% of ischemic strokes were attributed to cardioembolic events resulting from AF. Mortality was higher and the thirty day mortality was greater in AF strokes than in non-AF strokes (25% versus 14%).
AF also leads to cardiovascular function deterioration with loss of atrioventricular (AV) synchrony (a physiological condition of atrial electrical activity followed by ventricular electrical activity).
This can result in exertional fatigue and breathlessness. AF with a rapid ventricular rate can also lead to a tachycardia induced cardiomyopathy (reversible cause of heart failure and dilated cardiomyopathy) and heart failure. Importantly, AF is not only associated with the significant morbidity of heart failure and stroke, but also with a doubling effect on mortality.
Detection and assessment of AF patient
AF may be detected by a simple pulse examination, which reveals an irregular pulse. Automated blood pressure machines are now available with algorithms to detect AF based on pulse irregularity with reasonable diagnostic accuracy.
Technology and artificial intelligence (AI) have also improved the detection of AF with many consumer wearables (such as fitness trackers and smartwatches) and smartphones containing optical photoplethysmography (PPG) sensors to measure pulse rate. Based on a recently published Fitbit Heart Study, PPG-based software algorithms enhanced by AI detect irregular heart rhythms and identify undiagnosed AF in those who use wearables.
However, an ECG is needed to confirm the diagnosis of AF. Short-term recording with ambulatory 24 hours, 48 hours or even 7 days Holter may be useful but may not detect AF if it does not occur during the period of monitoring. In the past, event recorders have recorded only brief periods, but new wearable patch recorders provide prolonged ECG recording for 7-28 days.
According to a mSToPS study, it is found that continuous monitoring with a wearable ECG patch leads to higher rates of AF diagnosis and greater initiation of anti-coagulants. The new smartwatches from Apple, Samsung and Huawei have the ability to record a 30-second interval single lead ECG, which can help detect irregular pulse and alert the patient when there is an abnormality.
These can provide a good recording in about 80-90% of the patients, and the device can interpret the rhythm strip correctly about 80% of the time.
Screening for AF is beneficial in the older population (>65 years old), especially those with associated co-morbidities such as heart failure, hypertension, diabetes and cardiovascular disease. Certain patient groups, such as those with recent embolic stroke of uncertain source (ESUS) and transient ischemic attacks require more intensive monitoring for AF.
In such patients with extremely high risk and high likelihood for AF, an implantable loop recorder may be inserted over the left chest to continuously monitor the patient for as long as 3 years. In general, screening in these higher risk populations have shown a small net benefit compared to the usual standard of card.
Management of AF
Once the diagnosis of AF is confirmed, the patient can be risk stratified for stroke using the CHADSVASC score. Highrisk patients can be anti-coagulated, preferably with the DOAC, while patients with associated co-morbidities, especially hypertension, correctable precipitants (e.g, thyroid disease), structural heart disease, or pulmonary disease can be monitored closely.
Control of symptoms using rate or rhythm control can then be decided. Recent studies suggest that early rhythm control may be better and prevent progression to permanent AF. In selected patients whose rhythm cannot be controlled by simple anti-arrhythmic drugs, catheter ablation may be considered.
AF is increasing in prevalence and is associated with significant morbidity and even mortality. New technologies have improved the detection of AF. Once detected, risk stratification and correct management can then treat and prevent the progression of AF.
Article is contributed by Dr Teo Wee Siong, Consultant Cardiologist and Electrophysiologist in Private Practice.



