COVID-19: Truths and Myths About Blood Clots and Hypertension

The novel SARS-CoV-2 is now a global pandemic and both the healthcare services and patients have to adapt to limit the impact it has on chronic disease management.
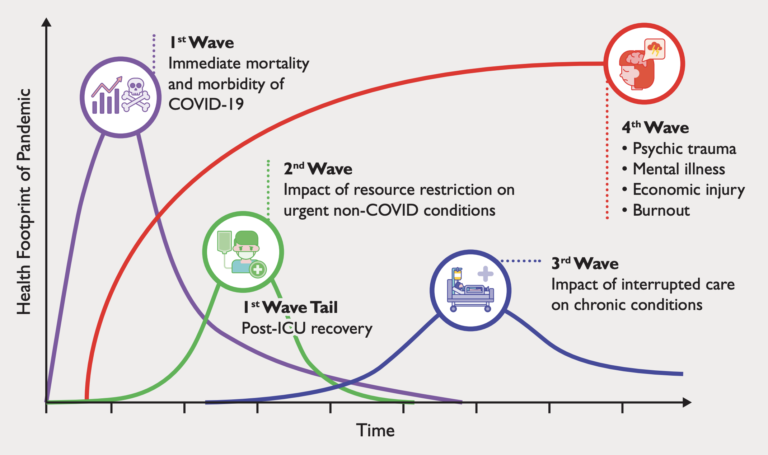
Singapore has done very well in reducing the first wave (immediate mortality and morbidity) when the SARSCoV-2 virus hit Singapore in February 2020. The system has been adapting rapidly to limit the impact on resource limitation and interruptions in care for chronic conditions in the second and third wave over these few months. While we watch out for our patients, we will also need to watch out for the fourth wave – mental stress and burnout of the healthcare workers and the economic impact on Singapore.
One contribution to unnecessary mental stress is the confusion caused by news on the formation of blood clot and hypertension drugs in relation to COVID-19 infected patients amongst physicians and the layperson public.
COVID-19 and blood clots
There is an emerging body of data which suggests that COVID-19 patients are predisposed to blood clot formation in both the venous and arterial systems at a higher frequency than seasonal flu. The exact mechanism is still not well understood. The frequency of blood clot is highest amongst patients who require critical care management which can cause complications like heart attacks, strokes and clots occurring in the venous system that can travel to the lungs. Although it has been reported as case series in other countries, in Singapore, we have fortunately not seen this phenomenal manifest in the majority of our patients infected with the SARCoV-2 virus.
Postulated mechanisms for the increased thrombotic risks include disruptions in vascular lining due to the interaction between SARS-CoV-2 and Angiotensin Converting Enzyme 2 (ACE2) receptor. The binding capacity of the SARS-CoV-2 spike protein to the ACE2 receptor is more than 10 times that of the SARS virus. This means it might be easier for SARS-CoV-2 to get into human cells, causing direct viral damage. Other mechanisms include invoking a fierce immune-mediated cytokine or coagulation response.
Physicians managing COVID-19 patients are always on the lookout for such complications. Although routine use of blood thinners is not recommended for all patients, prophylactic doses of blood thinners are used in severe cases that require intensive care.
Discharged COVID-19 patients should continue to watch out for symptoms of chest pains, leg swelling and recurrence of breathlessness as some of the thrombotic complications can occur in the recuperation phase.
COVID-19 and Hypertension
Due to the conflicting evidence on the precise role that ACE2 plays in SARS-CoV-2 infections, there were earlier reports linking the higher incidence of hypertensive patients for COVID-19 infections due to the possible interaction with anti-hypertensive medications. Major cardiology professional societies recommended against changing any hypertension medications, cautioning the potential harm when medications are interrupted. Since then, multiple observational publications in COVID-19 patients show no adverse outcomes in patients taking the two classes of blood pressure medications, angiotensin-converting enzyme inhibitors (ACEi) or angiotensin II receptor blockers (ARB) that can potentially increase ACE2 levels in cells. In fact, studies are underway to potentially use these antihypertensive medications as protective drugs against the adverse complications of COVID-19 patients if the Renin-Angiotensin-Aldosterone System (RAAS) – a hormone system within the body that is essential for the regulation of blood pressure and fluid balance – is disrupted.
Vulnerable to take extra precaution
What we do know now of the SARs-CoV-2 virus is that it can cause infections with a latent infectious asymptomatic period and often a mild respiratory disease in most patients. In the vulnerable group, particularly the elderly, those with chronic conditions like coronary artery disease, heart failure, hypertension, diabetes, active smokers or lung disease, the disease can be serious, and patients might need hospital care. We should do our part to reduce the rate of infection in the community with ongoing measures like masking up and social distancing. We should also stay away from public areas or vulnerable groups if we are feeling unwell.
As the pandemic goes on, we should continue to encourage one another and watch out for signs of stress and burnout during this period of adjustments.
Article is contributed by A/Prof Jack Tan, a member of the Singapore Heart Foundation’s Board of Directors. He is also the Deputy Head of Cardiology at the National Heart Centre Singapore and the Head of Cardiology at the Sengkang General Hospital.




